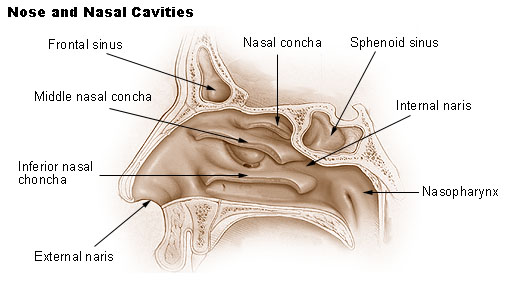
Nose and nasal cavities. Image source: Wikipedia, public domain.
{kind=link}
Recommendations for Management of Acute Bacterial Sinusitis by the Infectious Diseases Society of America (IDSA):
Bacterial rather than viral rhinosinusitis should be diagnosed when any of the following occurs:
- persistent symptoms lasting at least 10 days, without improvement
- symptoms or high fever and purulent nasal discharge or facial pain for 3–4 days at illness onset
- worsening symptoms after an initial respiratory infection, lasting 5–6 days, has started to improve.
Empirical therapy should be started as soon as acute bacterial rhinosinusitis is diagnosed clinically.
Amoxicillin-clavulanate, instead of amoxicillin alone, is recommended for both children and adults.
Macrolides and trimethoprim-sulfamethoxazole are not recommended as empirical therapy, because of high rates of antimicrobial resistance.
References:
Algorithm for the management of acute bacterial rhinosinusitis (figure)
Guideline Issued for Managing Acute Bacterial Rhinosinusitis - Physician's First Watch http://bit.ly/TGn6aM
IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults http://bit.ly/TGnaHB
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.