
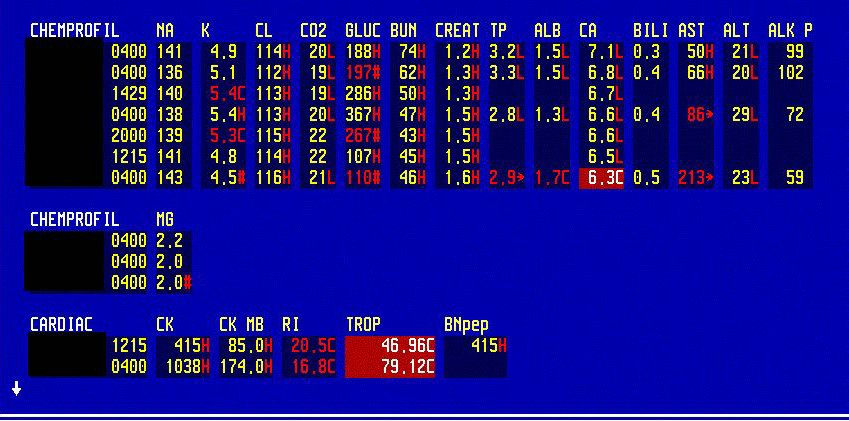
CBC in a patient with sepsis due to severe C. diff. colitis, CMP, CPP. Note the marked elevation in WBC, often seen in severe C. diff.

ABG and ventilator settings in a patient with septic shock who was successfully extubated.
Note the standard use of A/C (assist control ventilation) as the most common mode of ventilation.
After the weaning parameters were checked, the ventilation mode was switched to CPAP for 30 min. The patient tolerated CPAP very well and was extubated.
She became acutely SOB after extubation.
What do you think was going on?
With RSBI of less than 100, the chances for successful extubation are 85%.
There are only a few things that can spoil the picture: pulmonary edema, laryngeal edema with stridor and a lot of secretions.
The patient was suctioned repeatedly and put on BiPAP. Her condition improved within 2 hours and she maintained SpO2 96% on face mask. BiPAP was discontinued.
The sequence was A/C, then CPAP, then BiPAP, and finally face mask. In less complicated cases, the patient can tolerate face mask immediately after the intubation.
Final diagnosis: Respiratory failure in shock. An example of successful extubation strategy.
What did we learn from this case?
RSBI of less than 100 is the most important predictor of successful extubation.
When can you wean a patient off the ventilator?
-The original problem that caused the intubation has resolved or is stabilized.
-CVS is stable and the patient is off pressors.
-PaO2 is more than 60 on FiO2 of 40-60.
-RR less than 30
-MV more than 10 L
-RSBI less than 100. RSBI is RR/TV which means that the patient must have a low RR and a high TV

RSBI of less than 100 is a predictor of successful extubation
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.