PMH: Severe end-stage cardiomyopathy with an ejection fraction of 15%
Physical examination: Cachectic in NAD
VS 36.8-20-76-143/80
SpO2 96% on 2L
HEENT: mild JVD
Lungs: Harsh Velcro rales heard on the left almost to the scapula tip with a few rales at the right base
CVS: Heart sounds are distant
Abdomen: soft, nontender
Extremities: No c/c/e
CXR showed a progression of bilateral pulmonary infiltrates, especially on the right.

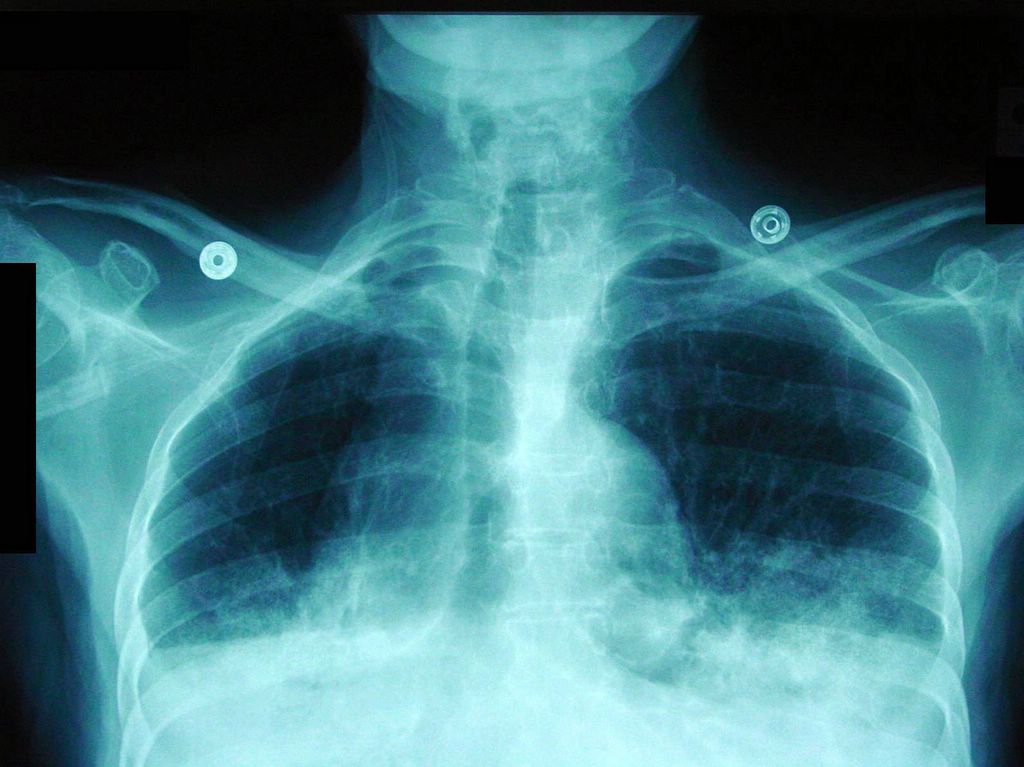

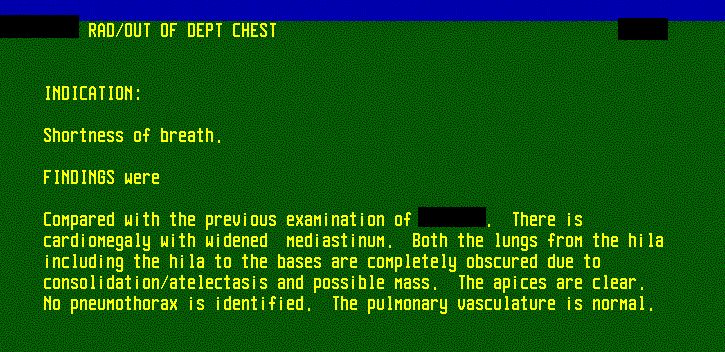
Bilateral bronchialveolar carcinoma; CXR report
What it looks like high diaphragms on this CXR actually is the fluid produced by this cancer. Half of the lungs are filled with this mucinous secretions. See how the trachea dives deep in the fluid - the carina is well below the fluid level.
The first biopsy done through bronchoscopy was inconclusive. The pulmonary consultant thought that the patient most likely had bronchoalveolar cell carcinoma and recommended transthoracic biopsy under CT guidance. The biopsy confirmed the clinical diagnosis.

Biopsy report
Final diagnosis: Bronchoalveolar cell carcinoma
What happened?
Her cancer was inoperable, she refused any further treatment and soon expired under hospice care.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.