PMH: HTN, COPD, CAD, DVT, mental retardation, blindness, pacemaker, facial cancer S/P excision
Medications: ASA, Lisinopril, Lopressor
SH: Smoker - 3 ppd for 18 years, quit 3 years ago
Physical examination:
WD/WN in NAD
VS 36.6-70-20-111/70
SpO2 100% on RA
Chest: (B) wheezing
CVS: Clear S1S2
Abdomen: Soft, NT, ND
Extremities: no c/c/e
What do you think is going on?
COPD
ACS
Bronchitis
And, of course, in every smoker with lung symptoms, lung cancer is among the differentials.
What tests would you order?
CBCD, CMP
CPP x 2 q 8 hr (he has chest pain after all)
EKG
CXR - and there was the surprise - a RML lung mass.
You know that the first questions is "Is that new?", so we checked the previous CXR done 2 years ago.

CXR done two years ago showed an implanted pacemaker.


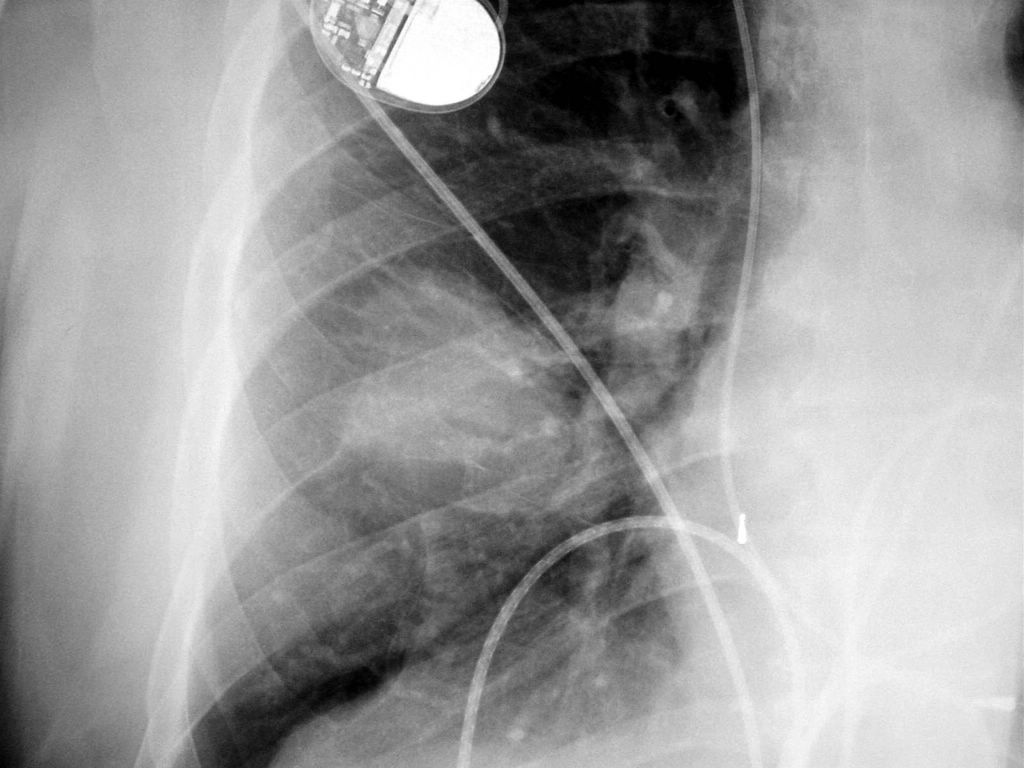
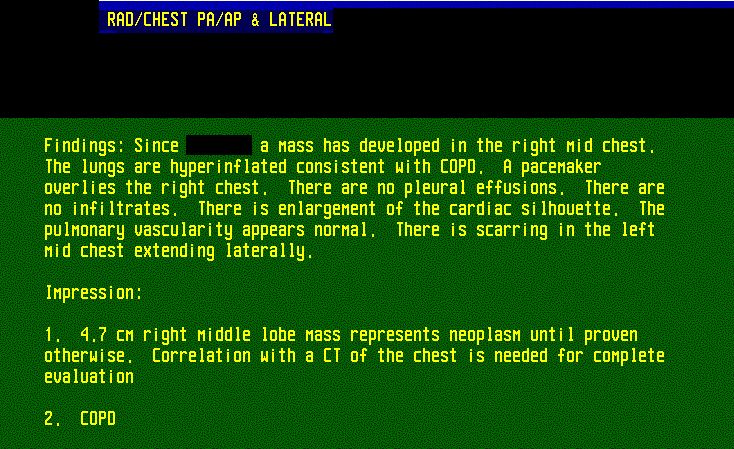
CXR during this admission shows a new 4.7 cm RML mass which is cancer until proven otherwise. Close-up of the mass. CXR report.
The next step, after the mass was diagnosed on the CXR, is to order a CT scan, and then to obtain a tissue diagnosis, e.g. to perform a biopsy.

CT of the chest





CT chest


CT chest
CT chest report:
Technique: Using 100 cc of nonionic intravenous contrast spiral CT of the chest was performed.
Findings:
Margining the right anterior pleural surface in the RML there is a 4.3 cm soft tissue mass that represents neoplasm until proven otherwise. The adjacent ribs appear intact.
There is cardiomegaly. A pacemaker is noted. There is opacification of numerous venous collaterals in the right chest wall. There is no mediastinal or hilar adenopathy.
Lung windows show signs of COPD. There is subpleural scarring in the left lung base and lingula. Except for the pleural based mass in the RML no other lesions are detected.
Impression:
1. 4.3 cm pleural based right middle lobe mass represents neoplasm until proven otherwise.
2. Mild COPD with slight parenchymal scarring
3. Cardiomegaly
4. Pacemaker
5. This report was faxed to the ordering physician at the time of dictation in addition to the standard method of sending the report.
What happened?
The patient's symptoms improved with aerosols and oral prednisone and he was discharged to his caregiver's home. He is scheduled to come back for an outpatient transthoracic biopsy.
CT scan of the abdomen and head were negative for any metastases.
Final diagnosis: RML mass, likely due to lung cancer. Biopsy to be done.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.