PMH: negative
Medications: none
Physical examination:
Ashen, ill-appearing male
V/S: 36.9-115-22-138/80
Chest: diminished breath sounds (B)
CVS: Tachycardic, clear S1S2
Extremities: Peripheral varicose veins, 1+ edema (B). No Homan's sign or calf tenderness.
What do you think is going on?
ACS?
PE?
Pericarditis?
What happened?
He was given ASA, nitroglycerin SL every 5 minutes x 3. His initial SpO2 was 89-90% on RA and he was put on 3 liters by NC. ABG was done.
ABG: pH 7.436, PaCO2 34, PaO2 90, SpO2 96% on 3 liters.
His perioral cyanosis improved, and he felt better.

ABG shows respiratory alkalosis. He was hypoxic on RA.
D-dimer was 5784.
CXR showed a shallow inspiration or low lung volumes. The lungs appeared clear.
With his positive D-dimer, his initial presentation of hypoxemia, and HR 114, this patient was a prime candidate for a pulmonary embolus.
A spiral CT of the chest was ordered, and it came back as positive for a bilateral main pulmonary artery emboli.
What happened next?
He was started on a heparin bolus and drip, and admitted to ICU. Coumadin was started.

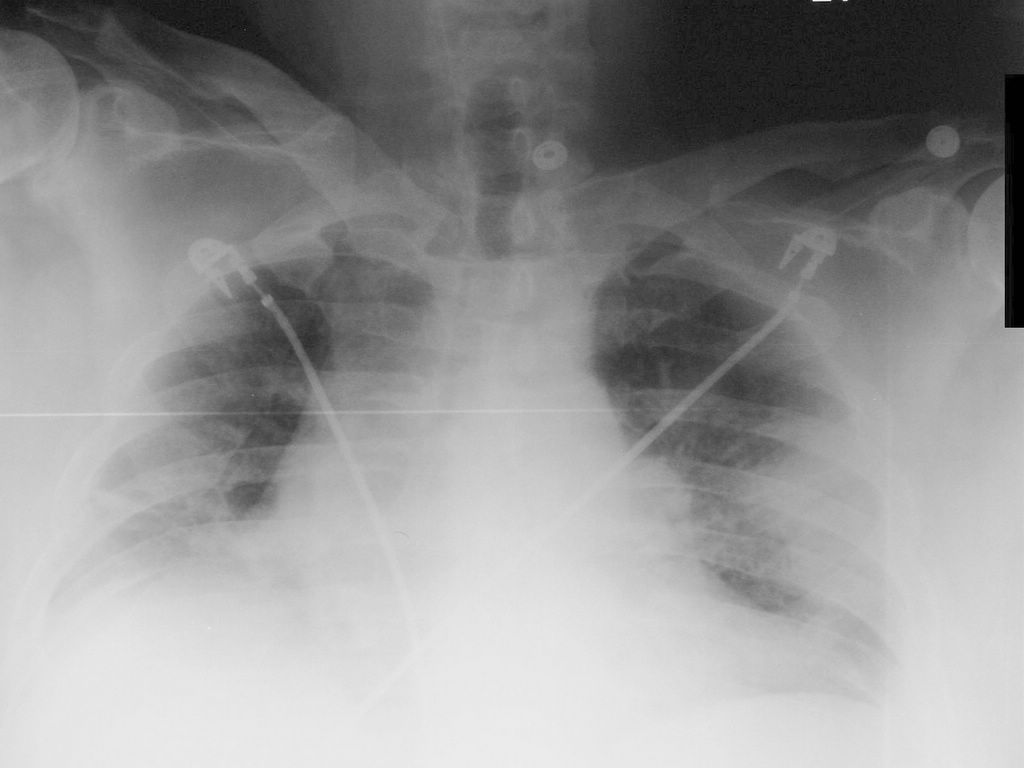
This is the initial CXR when the patient presented with PE. He was hypoxic and the spiral CT of the chest showed massive bilateral PE.
CXR done 3 days later showed a wedge-shaped peripheral lesion, seen better on the follow-up CXR done 3 days after that.
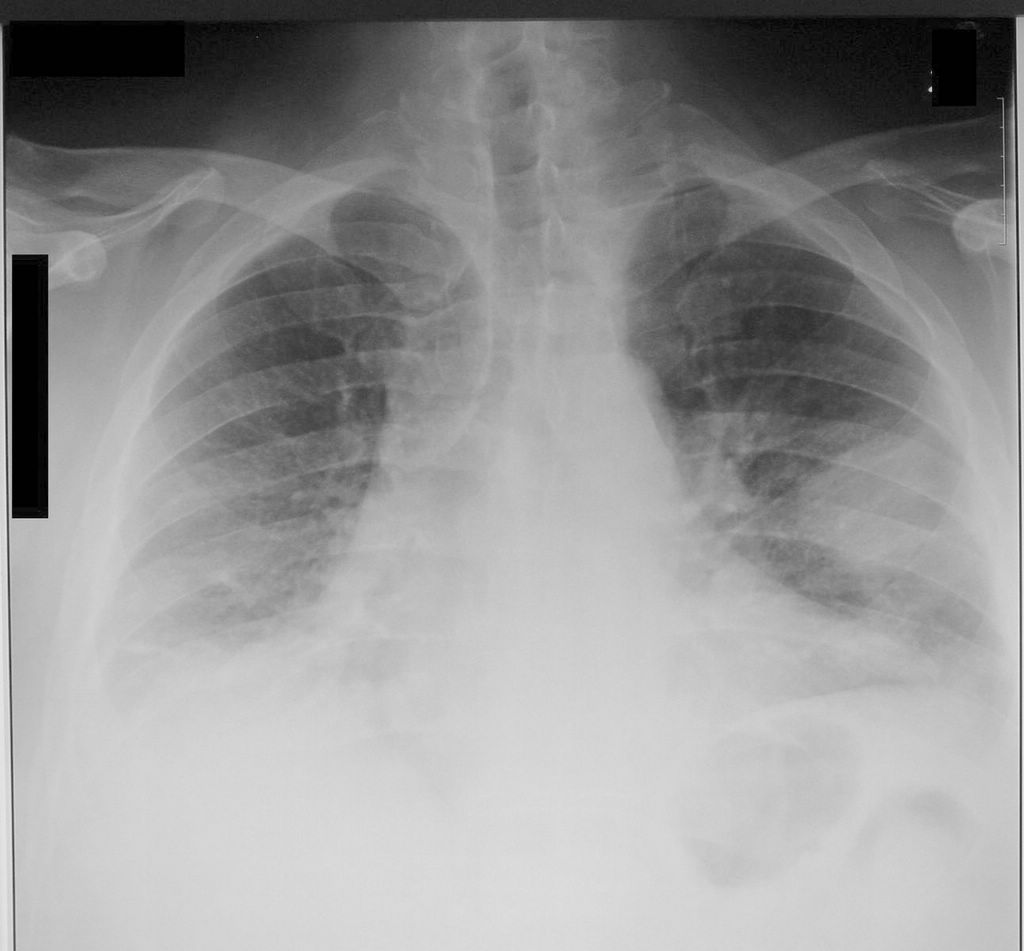


Third CXR, one week after the initial one. Close-up of the wedge-shaped peripheral lesion.
The classic radiographic finding of pulmonary infarction is a wedge-shaped, pleural based triangular opacity with an apex pointing toward the hilus (Hampton hump).
This is observed only infrequently.
Final diagnosis: Hampton hump (pulmonary infarction) in PE
References:
Pulmonary Embolus and Lung Infarction - FP Notebook.com
Acute Pulmonary Embolism (Helical CT) - eMedicine
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.