The patient has gradually being losing weight for the past two years (20 pounds), claiming that she was consciously trying to loose weight by eating less. She has had decreased appetite and lost 8 pounds over the last two months. She refused any work-up and her daughter agreed.
The patient denies dysphagia, heartburn, abdominal pain, or problems with her bowels; however, she does say that she has had piles with intermittent bleeding since she was 13 years old.
PM: HTN, CRI, Glaucoma, R eye blindness, HOH
Medications: Atenolol 25 mg po qd
SH: Denies smoking, drugs, or alcohol. Lives with her daughter.
Physical exam:
VSS, thin lady in NAD
Chest: CTA (B)
CVS: Clear S1S2
Abd: Soft, NT, ND, +BS
Rectal: FOBT negative
Ext: no c/c/e
Neuro: AAO x 3, non-focal
Urine sample taken in the ER showed gross hematuria which patient never reported or noticed before.
What do you think is going on?
Anemia die to GI bleed?
Anemia and weight loss in the elderly may indicate colon CA.
But why the hematuria?
Is it due to UTI?
What tests would you order?
CBCD, CMP
Of course, reticulocyte count and peripheral smear should be ordered because we are working-up anemia.
Fe profile and ferritin
INR/PTT
Type and screen 2U PRBC
UA
FOBT x 2
What happened?
She was admitted to the hospital and transfused 2U PRBC. After that her Hgb was stable.
GI consult was called but the patient refused any work-up including colonoscopy or CT of the abdomen. FOBT x 3 was negative and the iron profile showed anemia of chronic disease.
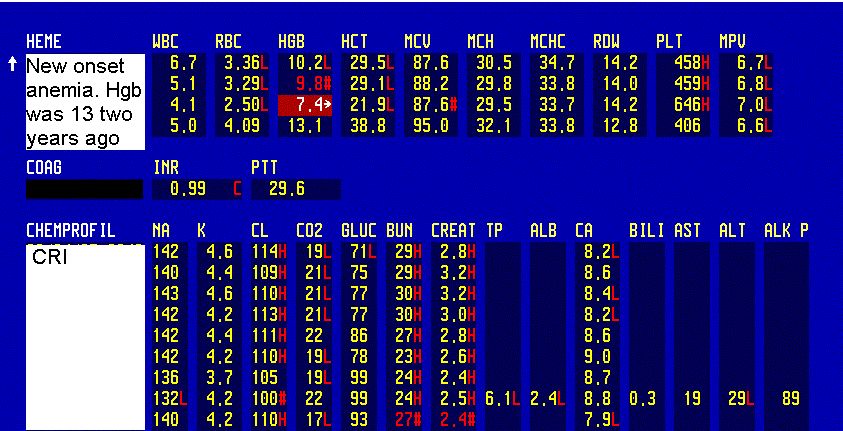



CBC, BMP; Iron profile shows ACD; Reticulocyte count and haptoglobin
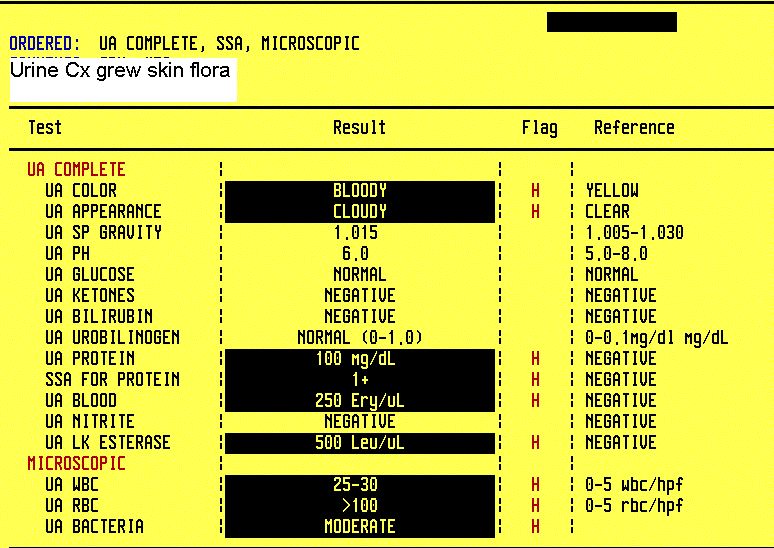
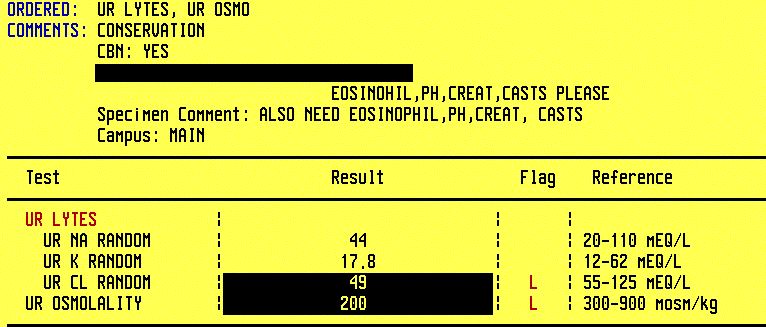
UA shows gross hematuria and bacteria; Urine electrolytes
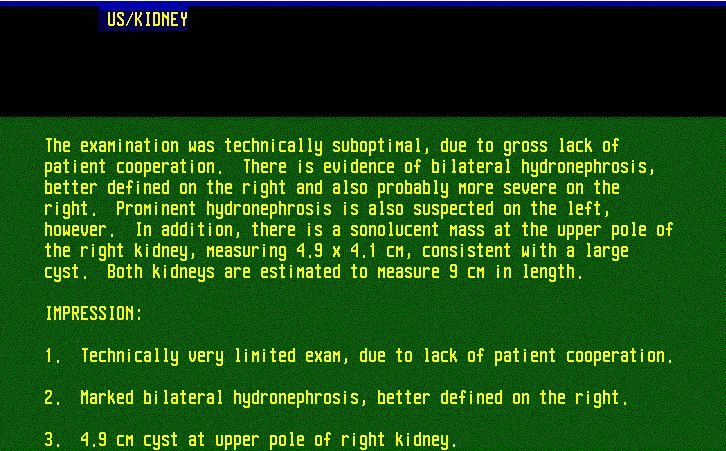
Kidney U/S revealed (B) hydronephrosis (report)
Urine continued to be bloody, and urology consult was requested, who arranged for a cystoscopy and bilateral retrograde pyelograms. The patient and the family agreed.
Mnemonic for Hematuria DDx=
T-SHIRTTT:
T U, e.g. bladder CA
S tone (nephrolithiasis)
H emophilia
I nfection (UTI)
R enal, e.g. GN
T rauma
T hrombocytopenia
T B
Cystoscopy:
The video-assisted cystoscopy demonstrated a large volume of bladder carcinoma, completely encompassing the bladder neck and obliterating the trigone such as the ureteral orifices were not identified, and extending up the right and left sidewall of the bladder toward the dome. Retrograde pyelograms was not possible.
Biopsy forceps were used to randomly biopsy several areas. These areas were fulgurated with the Bugbee electrode. A Foley catheter was inserted and the procedure was terminated after an examination under anesthesia demonstrated induration and possible fixation on the anterior vaginal wall.

Bladder biopsy showed bladder carcinoma (report)
What happened next?
Findings were discussed with the patient and family and oncology consult was called.
Epogen was started for the anemia.
The patient and her family were aware of the diagnosis and, after great discussion, the patient decided to proceed with the cystectomy, in spite of all risks discussed. She was medically cleared for the surgery and she had radical cystectomy with urinary diversion to an ileal loop.
Final diagnosis: Gross hematuria and weight loss due to bladder carcinoma
What did we learn from this case?
Ballder carcinoma is in the differential of hematuria, especially in the elderly patients. The standard work-up consists of ruling out UTI, kidney U/S and a cystoscopy.
Bear in mind that elderly patients may not report bloody urine due to visual impairment (like in this case) or dementia.
Bladder cancer screening is not recommended.
References:
Transitional bladder cell carcinoma - Path Guy.com
Bladder Cancer in Merck Manual
Bladder Cancer in eMedicine
Hematuria - clinical decision case - Cleveland Clinic
Evaluation of Asymptomatic Microscopic Hematuria in Adults - AFP 09/99
Hematuria DDx mnemonics - MedicalMnemonics.com
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.